Editorial Review
Author: Dr. Marcus Webb, Ph.D.(Ph.D. Molecular Pharmacology · Science Contributor)|Reviewed by: Scientific Compliance Reviewer
Last reviewed: June 2026
The incretin research landscape in 2026
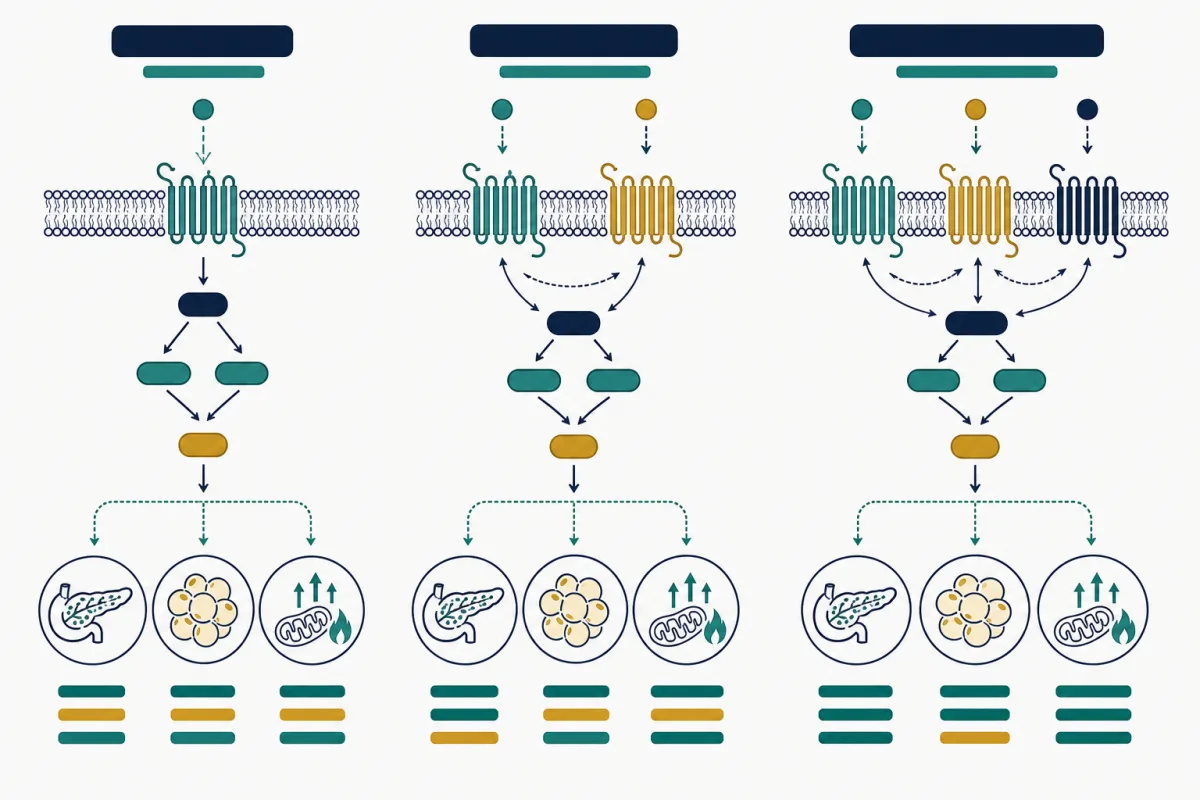
Three peptides dominate metabolic research conversation in 2026, and they form a clean mechanistic ladder: semaglutide targets one receptor, tirzepatide targets two, and retatrutide targets three. Understanding that progression is the fastest way to make sense of why each compound behaves differently in published studies and why research interest has shifted toward the multi-receptor agonists.
The shared foundation is the incretin system — the gut hormones that coordinate insulin secretion, appetite signaling, and energy handling after nutrient intake. The two incretin hormones of interest are GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide). Retatrutide adds a third axis by also engaging the glucagon receptor.
Why has research interest climbed the ladder toward more receptors? The short answer is that each added axis brings a mechanistically distinct lever on energy balance.
GLP-1 alone influences appetite and glucose-dependent insulin secretion; adding GIP introduces a second, partly independent metabolic input; adding glucagon-receptor agonism brings energy expenditure and hepatic lipid handling into play.
More levers mean more ways to move the system — but also more variables to characterize and more potential for off-target complexity. The progression is therefore as much about expanding the research toolkit as it is about chasing larger effects.
This comparison frames the three at the receptor level, summarizes the published trial context, and addresses the documentation realities that matter when sourcing any of them for research. It is RUO education and not medical, prescribing, or dosing advice. For a deeper single-compound view, see the GLP-1 research guide.
Semaglutide: the single GLP-1 agonist baseline
Semaglutide is a GLP-1 receptor agonist and the most clinically validated of the three by a wide margin, with a large body of human trial data behind its approved drug formulations. As a research compound, it serves as the mechanistic baseline against which the dual and triple agonists are measured.
At the receptor level, GLP-1 agonism is associated with glucose-dependent insulin secretion, slowed gastric emptying, and central appetite-signaling effects mediated in part through hypothalamic pathways. The "glucose-dependent" qualifier matters: because insulin release is tied to ambient glucose, the mechanism carries a different profile than insulin-secretagogues that act regardless of glucose level.
In published weight and metabolic research, semaglutide established the efficacy ceiling that later compounds aimed to exceed.
Its long history also means its characterization is the most mature — useful when a study needs a well-understood reference agonist rather than the largest possible effect size.
Research sourcing context is covered in the semaglutide sourcing guide and the semaglutide compound profile.
Tirzepatide: dual GIP/GLP-1 agonism
Tirzepatide engages two receptors: GIP and GLP-1. The rationale for dual agonism is that GIP and GLP-1 act through partially distinct but converging pathways, and engaging both may produce metabolic effects greater than GLP-1 agonism alone.
Head-to-head clinical research comparing tirzepatide against semaglutide has been a major story of the past few years, and the dual agonist generally demonstrated larger effects on weight and glycemic endpoints in those trials.
The GIP arm is the interesting variable. GIP's role is more nuanced than GLP-1's — its effects on insulin sensitivity, adipose handling, and appetite have been the subject of active mechanistic debate. What the trial data established is that, in combination with GLP-1 agonism, the dual approach produced a stronger metabolic signal than the single-receptor baseline.
For research selection, tirzepatide sits in a useful middle position: more potent effect signals than semaglutide in published comparisons, with a deeper data set than retatrutide. Sourcing and documentation context is in the tirzepatide research sourcing guide, the tirzepatide compound profile, and our tirzepatide vs semaglutide discussion.
Free Peptide Calculator
Calculate precise reconstitution volumes and dosages with our peptide calculator tool.
Retatrutide: triple GIP/GLP-1/glucagon agonism
Retatrutide is the newest and most mechanistically ambitious of the three, engaging three receptors: GIP, GLP-1, and glucagon. The addition of glucagon-receptor agonism is the conceptual leap.
Glucagon is often thought of only as the hormone that raises blood glucose, but at the receptor level it also influences energy expenditure and hepatic lipid handling — which is why a carefully balanced triple agonist is hypothesized to address fat loss through a pathway the dual and single agonists do not touch.
Published Phase II data for retatrutide generated significant attention for the magnitude of weight-related effects observed, positioning it at the frontier of incretin research. As an emerging compound, however, its long-term data set is the thinnest of the three, and dose-dependent gastrointestinal effects have been noted in the literature, consistent with the broader incretin class.
For research programs, retatrutide is the compound to study when the goal is the cutting edge of multi-receptor metabolic pharmacology — with the corresponding caveat that less accumulated evidence means more careful experimental design. See the retatrutide compound profile and the head-to-head pages tirzepatide vs retatrutide and retatrutide vs semaglutide.
Get Peptide Research Updates
New research, product launches, and exclusive offers. No spam.
Head-to-head: how the three compare
The table below summarizes the mechanistic and evidentiary differences relevant to research compound selection. Effect-magnitude language reflects general trends in published comparative trials of the corresponding approved drug formulations and should not be read as a guarantee of results in any specific research model.
| Attribute | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|
| Receptors engaged | GLP-1 | GIP + GLP-1 | GIP + GLP-1 + glucagon |
| Agonist class | Single | Dual | Triple |
| Relative effect signal (trials) | Baseline | Greater than semaglutide | Largest observed in Phase II |
| Depth of published data | Most mature | Substantial | Emerging |
| Distinct mechanism added | — | GIP axis | Glucagon / energy expenditure |
| Best research fit | Reference agonist | Potency with depth | Frontier pharmacology |
The practical read: potency and mechanistic breadth increase from left to right, while the maturity and volume of evidence decrease in the same direction. There is no single "best" compound — only the best fit for a given research question and tolerance for working at the edge of the evidence base.
Important Disclaimer
All products and information on this page are intended strictly for laboratory and scientific research use only. Not for human consumption. These statements have not been evaluated by the FDA.
Documentation, purity, and sourcing realities
All three are sold strictly as research materials, and all three are sequences where identity and purity verification are non-negotiable.
The larger and more complex the peptide, the more synthesis routes can introduce closely related impurities that a headline purity number alone may obscure.
For these compounds in particular, laboratories should review the actual HPLC chromatogram and the mass-spectrometry identity confirmation on a batch-specific COA — not just a stated percentage.
Pricing also diverges sharply across the three, generally tracking synthesis complexity: single-agonist material tends to be the most economical and triple-agonist material the most expensive. That makes price-per-milligram comparison across vendors especially valuable, since list prices alone can mislead when vial sizes differ.
PurePep Vital aggregates these signals rather than selling product. Compare research listings on the semaglutide, tirzepatide, and retatrutide offer pages, with live pricing and partner codes on the deals hub.
Live Alpha Labs is our top-rated tracked vendor for documentation transparency; PurePep readers can use code SOL for 10% off eligible research orders, with BluGen and Halo compared alongside.
Tolerability and the GI signal across the class
One pattern unites all three compounds in the published record: gastrointestinal effects are the dominant tolerability signal across the incretin class. Nausea, altered gastric emptying, and related GI responses appear consistently in trial data, and the literature generally describes them as dose-dependent and most pronounced during dose escalation.
For research interpretation, two points follow.
First, the GI signal is mechanistically expected — slowed gastric emptying is part of how GLP-1 agonism influences appetite, so it is intertwined with the effect being studied rather than a wholly separate side reaction.
Second, the multi-receptor agonists do not escape this pattern; retatrutide's Phase II data, for example, noted dose-dependent GI effects consistent with the class even as effect magnitudes were larger.
This matters for compound selection because a research model studying tolerability or escalation dynamics has different requirements than one studying maximal effect.
The class-wide nature of the GI signal also means it is a poor differentiator between compounds — the meaningful differences lie in receptor breadth and effect magnitude, not in whether GI effects occur.
None of this constitutes safety guidance for personal use; it is a summary of patterns reported in research literature.
Reading the trial data critically
Comparative claims about these three compounds are everywhere, and not all are well-grounded. A few principles help separate signal from marketing.
- Trial populations differ. Effect sizes from one study cannot be directly subtracted from another unless the populations, durations, and endpoints match. Cross-trial comparison is suggestive, not definitive.
- Approved-drug data is not research-material data. Most published efficacy evidence comes from finished pharmaceutical formulations. Research-grade material is a different product class, and effect sizes do not automatically transfer.
- "Newest" does not mean "best." Retatrutide's larger Phase II signals are genuinely notable, but a thinner long-term record is a real limitation for any program that needs durability data.
- Averages hide variance. Trial responders are averages; individual and model-level variation is substantial and is exactly what controlled research is designed to characterize.
Applied honestly, these principles point back to the same conclusion: the right compound is the one whose evidence base matches the research question, verified against real documentation. For the broader class context, see the fat-loss research peptide guide.
Choosing a compound for a research program
A simple decision framework follows from the mechanistic ladder:
- Need a well-characterized reference agonist? Semaglutide offers the deepest data and most mature characterization.
- Need stronger effect signals with a solid evidence base? Tirzepatide balances potency and depth through dual GIP/GLP-1 agonism.
- Studying frontier multi-receptor metabolic pharmacology? Retatrutide adds the glucagon axis, with the caveat of thinner long-term data.
Whatever the choice, three principles hold across all of them: anchor conclusions to peer-reviewed endpoints rather than vendor marketing, verify every batch against a real COA, and keep all work within research-use boundaries. None of these compounds is an approved therapy in research form, and none of this content constitutes medical or dosing advice.
To go deeper, continue with the GLP-1 research guide, the fat-loss research peptide overview, or the weight-management research guide. For reconstitution math, the peptide calculator handles volumes without offering dosing recommendations.
Important Disclaimer — For Research Use Only
The information provided is for educational and research purposes only. All peptides discussed or linked on this site are intended strictly for laboratory and scientific research use only (RUO) and are not for human consumption, injection, ingestion, or any therapeutic application. These products have not been evaluated or approved by the FDA or any regulatory body and are not intended to diagnose, treat, cure, or prevent any disease or condition. Reliance on this content is at your own risk. Consult qualified professionals for any health-related decisions. PurePep Vital disclaims all liability for misuse. Products are offered by third-party retailers for research use only.
PurePep Vital is an editorial publisher, vendor comparison resource, and affiliate deal tracker. We do not manufacture, compound, sell, ship, test, prescribe, or handle peptide products. Purchases are completed directly through third-party retailers. PurePep Vital is not a compounding pharmacy or chemical compounding facility as defined under 503A of the Federal Food, Drug, and Cosmetic Act. PurePep Vital is not an outsourcing facility as defined under 503B of the Federal Food, Drug, and Cosmetic Act.
Disclosure: This page contains affiliate links. We may earn from qualifying purchases. See our full disclosure.
Need deals after the research?
Use the deals hub to compare current offers, partner codes, and research news. We recommend retailers that provide quality signals when available.
Explore Our Guides
Related Articles

Tirzepatide vs Semaglutide: Reddit Discourse vs Published Research (2026)
Social channels amplify incretin peptide discussions; this article contrasts Reddit narratives with trial-published endpoints for research literacy.

Retatrutide Peptide: Triple Incretin Research and Trial Context
Retatrutide simultaneously activates GIP, GLP-1, and glucagon receptors. Published Phase II trials report substantial dose-dependent weight reduction in study participants—here is the research landscape for laboratories comparing incretin-class molecules.
Tirzepatide Peptide: Dual-Action GLP-1 Research
Tirzepatide is the first dual GIP/GLP-1 receptor agonist, combining two incretin pathways for unprecedented metabolic effects. Here is what the clinical data reveals.
Best Peptides for Fat-Loss Research in 2026: A Mechanism-First Guide
Fat-loss peptide research falls into three mechanistic families. This guide organizes the most-studied 2026 compounds by how they work, summarizes the evidence, and explains how laboratories evaluate documentation before sourcing.
Frequently Asked Questions
They engage progressively more receptors: semaglutide is a single GLP-1 agonist, tirzepatide is a dual GIP/GLP-1 agonist, and retatrutide is a triple GIP/GLP-1/glucagon agonist. Potency signals generally increase across that ladder, while the depth of published data decreases.